Introducing the BODi® Partner Podcast, the official podcast channel devoted exclusively to BODi Partners. From archives of the BODi Wake-Up Call, I Am BODi stories, and What I Know Now success tips from seasoned Partners, this podcast is your one-stop source for personal development, business training and peer-to-peer inspiration. Ready to explode your business? Tune in regularly to our official podcast and join the ranks of those transforming their lives and the lives of others!
…
continue reading
Το περιεχόμενο παρέχεται από το CardioNerds. Όλο το περιεχόμενο podcast, συμπεριλαμβανομένων των επεισοδίων, των γραφικών και των περιγραφών podcast, μεταφορτώνεται και παρέχεται απευθείας από τον CardioNerds ή τον συνεργάτη της πλατφόρμας podcast. Εάν πιστεύετε ότι κάποιος χρησιμοποιεί το έργο σας που προστατεύεται από πνευματικά δικαιώματα χωρίς την άδειά σας, μπορείτε να ακολουθήσετε τη διαδικασία που περιγράφεται εδώ https://el.player.fm/legal.
Παρόμοιες με Cardionerds: A Cardiology Podcast
We are often distracted in life and never really dive deep into the real foundation of self improvement, goal achieving, and wellbeing. - Join our team of experts every week as we discuss the real facets of manhood. Topics like: How to develop more self esteem, self love, deeper relationships. How to improve our wellbeing, mental toughness, resilience, and productivity. How to develop critical skills, become better leaders, expand our careers/business, create financial security and contribut ...
…
continue reading
Although the world is becoming mostly sedentary, our bodies still require a wide variety of daily movements in order to work well. Many of us struggle to get regular exercise, but even that can fall short of nourishing the body from head to toe. How can we move more—a lot more—when we have sore, stiff parts and overly busy lifestyles? Join Katy Bowman M.S., biomechanist, author, and movement educator as she combines big-picture lessons on biomechanics, kinesiology, physiology, and natural hu ...
…
continue reading
For the complete newbie or the experienced hypnotist, Brain Software with Mike Mandel is the world's most interesting, educational and fun podcast discussing hypnosis, NLP and strategies for peak performance and self improvement. Mike Mandel is a 6-time award winning hypnotist, immensely popular keynote speaker, stage performer, psychotherapist and NLP trainer. He has been doing hypnosis since he was 12 years old. Mike has an amazing ability to demystify hypnosis, teach core concepts, and te ...
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
Practical herbalism from practicing herbalists. Conversations, botanical deep-dives, Q&A with clinical herbalists Katja Swift & Ryn Midura of CommonWealth Holistic Herbalism.
…
continue reading
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Welcome to Almost 30 - a supportive space to fuel your conscious evolution. Join us, LA-based best friends Krista Williams and Lindsey Simcik, for heart-centered, hilarious conversations and real, raw, impactful interviews with brilliant guests. We dive deep into topics like modern spirituality to health and wellness, aliens to entrepreneurship, social justice, and self development. With every episode, our mission is to empower you, expand what you think is possible and, make you laugh - a l ...
…
continue reading
Short guided meditations to calm your anxiety, overcome negative thinking, increase your confidence, and more. Don’t think you have the time, or mental focus, to meditate? Most of these mind-shifting meditations are 10 minutes or less. Soothe your stress away and feel better fast with this award winning guided meditation podcast by Hypnotherapist Chel Hamilton today. For more information visit: https://meditationminis.com (https://meditationminis.com/) Please Note: The meditations presented ...
…
continue reading
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
Player FM - Εφαρμογή podcast
Πηγαίνετε εκτός σύνδεσης με την εφαρμογή Player FM !
Πηγαίνετε εκτός σύνδεσης με την εφαρμογή Player FM !

))
384. Case Report: Little (a), Big Deal – National Lipid Association
Manage episode 433043550 series 2585945
Το περιεχόμενο παρέχεται από το CardioNerds. Όλο το περιεχόμενο podcast, συμπεριλαμβανομένων των επεισοδίων, των γραφικών και των περιγραφών podcast, μεταφορτώνεται και παρέχεται απευθείας από τον CardioNerds ή τον συνεργάτη της πλατφόρμας podcast. Εάν πιστεύετε ότι κάποιος χρησιμοποιεί το έργο σας που προστατεύεται από πνευματικά δικαιώματα χωρίς την άδειά σας, μπορείτε να ακολουθήσετε τη διαδικασία που περιγράφεται εδώ https://el.player.fm/legal.
CardioNerds Dan Ambinder and Dr. Devesh Rai join cardiology fellows and National Lipid Association lipid scholars Dr. Oby Ibe from Temple University and Dr. Elizabeth Epstein from Scripps Clinic. They discuss a case involving a patient with elevated Lp(a). Dr. Jessica Pena provides expert commentary. Drs. Oby Ibe and Elizabeth Epstein drafted notes. CardioNerds Intern Christiana Dangas engineered episode audio. This episode is part of a case reports series developed in collaboration with the National Lipid Association and their Lipid Scholarship Program, with mentorship from Dr. Daniel Soffer and Dr. Eugenia Gianos.
An asymptomatic 34-year-old female presented to the cardiology clinic for cardiovascular risk assessment. Her past medical history included polycystic ovarian syndrome (PCOS) and depression. Her labs were notable for total cholesterol 189 mg/dL, LDL of 131 mg/dL, HDL 34 mg/dL, triglycerides 134 mg/dL, and Lp(a) 217 nmol/L. Her 10-year ASCVD risk by the PREVENT calculator was 0.5%, and her 30-year risk was 3.5%. She had no carotid plaque. Because her 30-year risk was significantly increased by her elevated Lp(a), intensive risk factor management was emphasized, and she was started on a low-dose statin with a plan to follow the patient to reassess the need for intensification of lipid-lowering and/or initiation of novel Lp(a)-lowering therapies over time.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
Pearls – Little (a), Big Deal – National Lipid Association
- You are never too young to see a preventive cardiologist! The field of preventive cardiology is shifting focus towards the identification of early upstream risk and intervention before the development of clinical ASCVD (1,5). Patients who have a strong family history of cardiovascular disease, a personal history of CVD at an early age, multiple risk factors, or genetic disorders such as familial hypercholesterolemia especially benefit from early cardiovascular risk assessment and reduction.
- Female-specific risk factors to incorporate into a young woman’s cardiovascular risk assessment include polycystic ovarian syndrome, hormone contraceptive use, early menarche (age <10 years old), primary ovarian insufficiency, fertility therapy, hypertensive disorders of pregnancy (eclampsia, preeclampsia, gestational hypertension, preterm delivery, gestational diabetes, multi-parity >5 pregnancies), early menopause (age <45 years old), & post-menopausal hormone therapy.
- Lp(a) testing for all! The most recent NLA scientific statement on the use of Lp(a) in clinical practice recommends measuring Lp(a) at least once in every adult for risk stratification.
- While Lp(a) has not yet been incorporated into our risk calculators, we do know that elevated Lp(a) increases 10-year risk. The European Atherosclerosis Society published a consensus statement on Lp(a), which includes a handy table to quantify the degree to which a patient’s 10-year risk increases as Lp(a) increases.
- Lifestyle changes are the first line and can reduce the risk of high Lp(a) by 66%. Next, we can consider the risks and benefits of LDL-lowering in a young patient and monitor closely for the development of plaque over time. Lp(a) lowering drugs such as olpasiran are on the horizon, and we can keep this patient in mind as a potential candidate for therapy in the future.
Notes – Little (a), Big Deal – National Lipid Association
When should patients see a preventive cardiologist?
- Strong family history of cardiovascular disease – A positive family history of CVD was defined as a self‐reported diagnosis of CVD in parents, siblings, or children that occurred at 60 years or younger. A positive family history of CVD is an independent predictor of both myocardial infarction and stroke. Among individuals with hypertension, family history of CVD has been shown to be independently associated with mortality by ischemic heart disease and family history of CVD mortality with incidence of overall CVD. Family history of CVD modifies future CVD risk depending on the number and age of affected first-degree relatives. Siblings of patients with CVD have about a 40% risk increase, while offspring of parents with premature CVD have a 60% to 75% risk increase.
- Personal history of early CVD – A personal history of cardiovascular disease at an age younger than 60 years. For young and middle-aged adults, increases in heart disease between 2020 and 2021 explain more than 4% of the most recent shortening in life expectancy. In particular, hypertensive heart disease, heart failure, and endocarditis have increased in young adults, particularly among Black individuals, through 2018. Consequently, young adults make up a growing proportion of cardiovascular disease events, with the proportion of premature myocardial infarction among adults younger than 40 years increasing by 2% every year. The increasing event rates observed among younger adults can be attributed to the increasing prevalence and onset of risk factors such as obesity and hypertension at younger ages, which exacerbate cumulative exposure and cardiovascular disease risk over near- and long-term time horizons.
- Multiple cardiovascular risk factors – Risk factors include hyperlipidemia, high triglycerides, elevated lp(a), diabetes mellitus, obesity, tobacco use, unhealthy diet, and lack of physical activity. Unadjusted event rates were 8-fold to 30-fold higher in persons with adverse levels of risk factor exposure during young adulthood (age 20–39 years) compared with persons with optimal levels of exposure.
- Familial hypercholesterolemia – In primary prevention, patients with FH had incidences of ASCVD and coronary heart disease (CHD) of 14.9/1000 and 5.8/1000 person-years, respectively, compared to 7.1/1000 and 2.1/1000 person-years in the normolipidemic group. FH conferred a hazard ratio (HR) of 7.1 and 16.7 for ASCVD and CHD, respectively, in patients younger than 35 years. In secondary prevention, patients with FH had incidences of ASCVD and CHD of 89.7/1000 and 34.5/1000 person-years, respectively, compared to 90.9/1000 and 28.2/1000 person-years in the normolipidemic group
What are some female-specific risk factors for cardiovascular disease? (7)
- PCOS – Polycystic ovarian syndrome (PCOS) is a disorder characterized by hyperandrogenism and menstrual irregularities. Women affected by PCOS have a heightened risk of developing diabetes due to associated insulin resistance, central obesity, and hypertension. This adverse cardiovascular risk profile in women with PCOS may lead to premature atherosclerosis (8,20). Women with PCOS have been shown to have an increased risk for CVD events (21).
- Depression — Among 593,616 young adults (aged 18–49 years) from 2017 to 2020, depression was independently associated with CHD and suboptimal cardiovascular health (CVH), with a dose‐response relationship (CVH was determined using 7 cardiovascular risk factors: hypertension, hypercholesterolemia, overweight/obesity, current smoking, diabetes, physical inactivity, and inadequate fruit and vegetable intake) (13). Suboptimal CVH was defined as the presence of ≥2 of these 7 cardiovascular risk factors, whereas optimal CVH was 0 or 1 cardiovascular risk factor.
- Early menarche – Results from the Women’s Ischemia Syndrome Evaluation (WISE) study demonstrated that in comparison to women with menarche at age 12 years, there was an approximately 4-fold adjusted increased risk for major adverse cardiac events for menarche ≤ 10 years (15).
- African descent – Safford et al. found that among those at the highest CHD risk, Black women’s hyperlipidemia was the least likely to be treated or controlled. Lp(a) is significantly higher among Blacks versus Whites, and in both, increased Lp(a) correlates positively with LDL-C and negatively with triglycerides. Another study based on the MESA population demonstrated that Black participants showed a significant risk of CHD in those with Lp(a) levels ≥ 75 nmol/L as opposed to White and Hispanic participants who had a greater risk with Lp(a) levels ≥125 nmol/L.
- Elevated BMI – Obesity and higher measures of central adiposity are associated with significantly higher rates of CAD, CVD mortality, sudden cardiac death, heart failure, and arrhythmias (23). High BMI accounted for 4.0 million deaths in 2015, more than two-thirds of which were caused by cardiovascular disease. Marked increases in obesity prevalence among adolescents over the past 35 years ultimately contribute to CVD risk into young adulthood.
Who should be getting an Lp(a) measured?
- Per the most NLA-focused update to the 2019 scientific statement on the use of Lp(a) in clinical practice, we now have sufficient evidence to support measuring Lp(a) at least once in all adults for risk stratification.
What risk calculators would apply to a young adult?
- The American Heart Association recently released the PREVENT calculator (c-statistic 0.72) for 10- and 30-year risk estimation of total CVD (composite of atherosclerotic CVD and heart failure) in primary prevention patients (10). This improves upon the prior pooled cohort equation because it is based on newer data from a larger, more diverse sample (6,612,004 US adults 30 to 79 years of age) than the existing tool. The calculator also takes into account other health conditions, such as cardiovascular-kidney-metabolic risk factors, adjusts for competing risk of non-CVD death, and incorporates an indicator of social determinants of health. Race was not included because it is a social construct, not a biological risk factor, and could, therefore, create bias. Three research teams were awarded $150,000 from AHA to further study how the risk calculator performs among people of various ages, racial and ethnic backgrounds, locations, and socioeconomic levels.
- A universal calculator (c-statistic 0.747 and 0.691 for patients with and without CAD) was also recently published in JACC. This was unique because it can be used in patients both with and without CAD, doing away with the concepts of primary vs secondary prevention and placing everyone on the same spectrum of risk. The calculator incorporates ASCVD vs no ASCVD, age, diabetes, SBP, HTN treatment, TC, smoking history, CRP, NT Pro-BNP, hs Troponin T and provides a 5- and 10-year risk of MACE. The calculator was able to identify patients without CAD who had a higher risk than those with prior CAD. This calculator is not yet available online, but the authors did publish their formulae, which can be plugged into Excel to create a calculator. Unfortunately, this calculator may not apply to our patient because it was validated in a cohort of patients aged 45-64 years.
- QRISK3 (c-statistic 0.75) has been validated in patients aged 25-84 years, so it can be useful in predicting cardiovascular disease in both younger and older patients. It also incorporates a wider variety of risk-enhancing factors than most other calculators, including diagnosis of HIV/AIDS, inflammatory diseases, CKD stage, type 1 and type 2 diabetes, and erectile dysfunction. However, it is important to note that this calculator was validated in a primarily European population, and the risk prediction may not be as accurate in other ethnic groups.
How does elevated Lp(a) influence a patient’s 10-year risk, and can we quantify it?
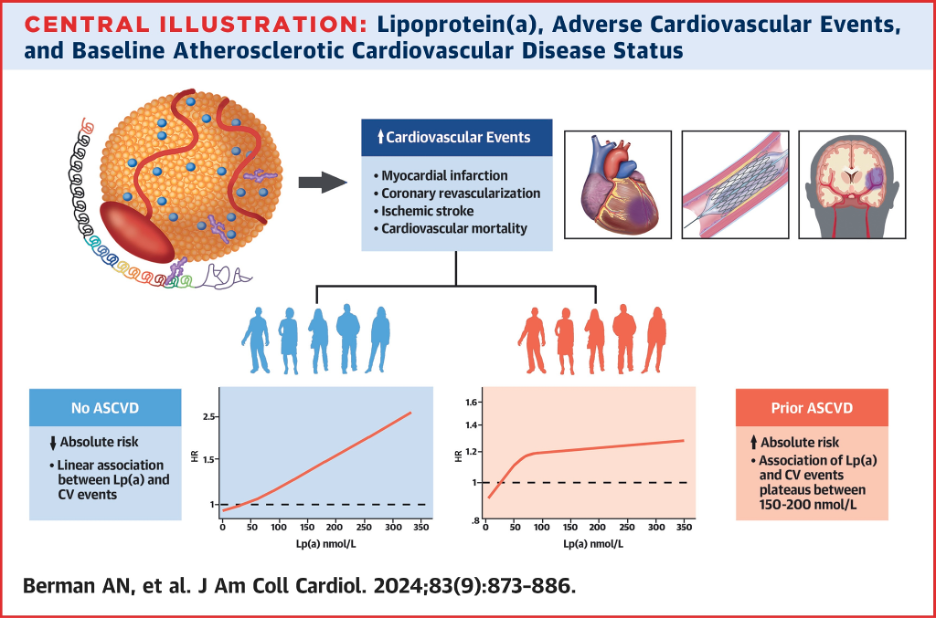
- A recent observational study demonstrated that elevated Lp(a) is associated with long-term MACE in both patients with and without cardiovascular disease. Among patients with ASCVD, individuals in the 71st to 90th percentile group had a 21% increased hazard of MACE (adjusted HR: 1.21; P < 0.001), and among patients without ASCVD, individuals in the 91st to 100th Lp(a) percentile group had the highest relative risk with an adjusted HR of 1.93 (P < 0.001). In patients without ASCVD, there was a linear association between Lp(a) and CV events, whereas in patients with prior ASCVD, the association plateaued between 150-200 nmol/L.
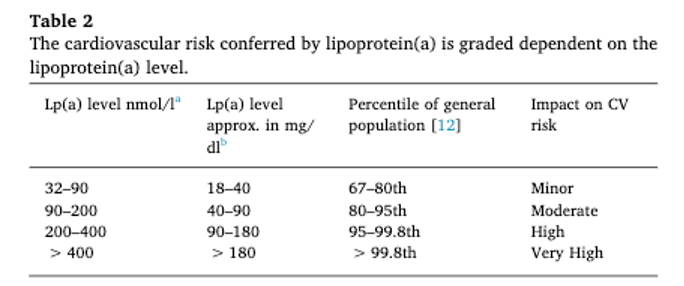
- Similarly, the 2019 consensus statement from HEART UK categorized the impact of CV risk associated with Lp(a) as minor, moderate, high, or very high based on the level of Lp(a). The table from this paper is a clinically useful tool to categorize risk from Lp(a).
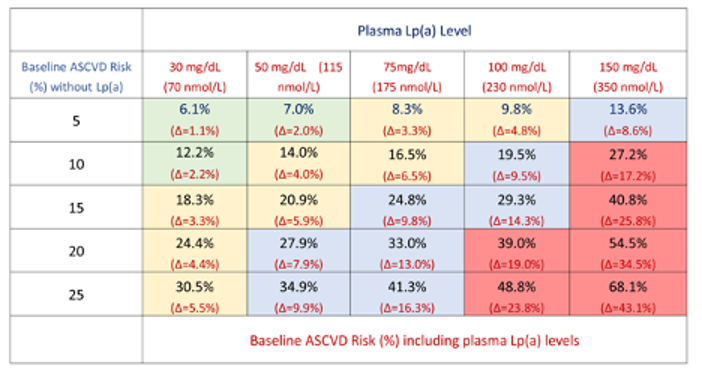
- The European Atherosclerosis Society has published a consensus statement on Lp(a) in the European Heart Journal which includes another useful table to adjust a patient’s 10-year risk based on the Lp(a) level(12).
How do we manage a young patient with elevated Lp(a)? Which patients might benefit from treatment with emerging Lp(a)-lowering therapies?
- Given we do not yet have Lp(a) lowering therapies available for clinical use, the mainstay of management for patients with elevated Lp(a) is intensive risk factor management. Beyond the question of LDL lowering, we know that lifestyle change plays a big role in patients with elevated Lp(a) specifically. While it was previously thought that lifestyle has no impact on ASCVD risk associated with elevated Lp(a), in fact, it very much does. It doesn’t lower Lp(a) directly but following the AHA Life’s Simple 8 lowers the risk of Lp(a) by 66%.
- There is some newer data suggesting that in patients with coronary artery disease, aggressive LDL lowering down to 50 can reduce the risk of Lp(a) by up to 50% (6). LDL of 50 mg/dL is a pretty aggressive treatment goal, which makes sense in very high-risk patients with existing CAD. However, we still need more data to guide LDL treatment goals in young patients(18).
- Novel Lp(a)-lowering therapies such as olpasiran are currently in clinical trials (19). We await the data from these trials in order to understand which patients would benefit most from treatment.
References
Allen N, Wilkins JT. The Urgent Need to Refocus Cardiovascular Disease Prevention Efforts on Young Adults. JAMA. 2023;329(11):886-887. doi:10.1001/jama.2023.2308
https://jamanetwork.com/journals/jama/fullarticle/2802264
Baber, Usman, Roxana Mehran, Samantha Sartori, Mikkel Malby Schoos, Henrik Sillesen, Pieter Muntendam, Mario J. Garcia, et al. 2015. “Prevalence, Impact, and Predictive Value of Detecting Subclinical Coronary and Carotid Atherosclerosis in Asymptomatic Adults: The BioImage Study.” Journal of the American College of Cardiology 65 (11): 1065–74.
https://pubmed.ncbi.nlm.nih.gov/25790876
Bhatia, H. S., Trainor, P., Carlisle, S., Tsai, M. Y., Criqui, M. H., DeFilippis, A., & Tsimikas, S. (2024). Aspirin and Cardiovascular Risk in Individuals With Elevated Lipoprotein (a): The Multi‐Ethnic Study of Atherosclerosis. Journal of the American Heart Association, 13(3), e033562.
https://www.ahajournals.org/doi/10.1161/JAHA.123.033562
Coll, B., Betriu, A., Feinstein, S. B., Valdivielso, J. M., Zamorano, J. L., & Fernandez, E. (2013). The role of carotid ultrasound in assessing carotid atherosclerosis in individuals at low-to-intermediate cardiovascular risk. Revista Española de Cardiología (English Edition), 66(12), 929-934.
https://pubmed.ncbi.nlm.nih.gov/24774105
Devesa, A, Ibanez, B, Malick, W. et al. Primary Prevention of Subclinical Atherosclerosis in Young Adults: JACC Review Topic of the Week. J Am Coll Cardiol. 2023 Nov, 82 (22) 2152–2162.
https://www.jacc.org/doi/10.1016/j.jacc.2023.09.817
Dykun, Iryna, Jürgen Kampf, Tienush Rassaf, and Amir A. Mahabadi. 2023. “Interaction between Elevated Lipoprotein(a) and LDL Cholesterol on Mortality Risk in Patients with Coronary Artery Disease.” European Journal of Preventive Cardiology 30 (13): e64–65.
https://academic.oup.com/eurjpc/article-abstract/30/13/e64/7065497?redirectedFrom=PDF
Elder P, Sharma G, Gulati M, Michos ED. Identification of female-specific risk enhancers throughout the lifespan of women to improve cardiovascular disease prevention. Am J Prev Cardiol. 2020;2:100028. Published 2020 Jun 6. doi:10.1016/j.ajpc.2020.100028
https://www.sciencedirect.com/science/article/pii/S2666667720300283
Glintborg D, Rubin KH, Nybo M, Abrahamsen B, Andersen M. Cardiovascular disease in a nationwide population of Danish women with polycystic ovary syndrome. Cardiovasc Diabetol. 2018;17(1):37. Published 2018 Mar 8. doi:10.1186/s12933-018-0680-5
https://pubmed.ncbi.nlm.nih.gov/29519249
Guan, W., Cao, J., Steffen, B. T., Post, W. S., Stein, J. H., Tattersall, M. C., … & Tsai, M. Y. (2015). Race is a key variable in assigning lipoprotein (a) cutoff values for coronary heart disease risk assessment: the Multi-Ethnic Study of Atherosclerosis. Arteriosclerosis, thrombosis, and vascular biology, 35(4), 996-1001.
https://pubmed.ncbi.nlm.nih.gov/25810300
Khan, S. S., Coresh, J., Pencina, M. J., Ndumele, C. E., Rangaswami, J., Chow, S. L., … & American Heart Association. (2023). Novel prediction equations for absolute risk assessment of total cardiovascular disease incorporating cardiovascular-kidney-metabolic health: a scientific statement from the American Heart Association. Circulation, 148(24), 1982-2004.
https://www.ahajournals.org/doi/10.1161/CIR.0000000000001191
Kolber MR, Scrimshaw C. Family history of cardiovascular disease. Can Fam Physician. 2014;60(11):1016.
Kronenberg, Florian, Samia Mora, Erik S. G. Stroes, Brian A. Ference, Benoit J. Arsenault, Lars Berglund, Marc R. Dweck, et al. 2022. “Lipoprotein(a) in Atherosclerotic Cardiovascular Disease and Aortic Stenosis: A European Atherosclerosis Society Consensus Statement.” European Heart Journal 43 (39): 3925–46.
https://pubmed.ncbi.nlm.nih.gov/36036785
Kwapong YA, Boakye E, Khan SS, et al. Association of Depression and Poor Mental Health With Cardiovascular Disease and Suboptimal Cardiovascular Health Among Young Adults in the United States. J Am Heart Assoc. 2023;12(3):e028332. doi:10.1161/JAHA.122.028332
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9973664
Lau, F. D., & Giugliano, R. P. (2022). Lipoprotein (a) and its significance in cardiovascular disease: a review. Jama Cardiology.
https://pubmed.ncbi.nlm.nih.gov/35583875
Lee, J. J., Cook‐Wiens, G., Johnson, B. D., Braunstein, G. D., Berga, S. L., Stanczyk, F. Z., … & Shufelt, C. L. (2019). Age at menarche and risk of cardiovascular disease outcomes: findings from the National Heart Lung and Blood Institute‐sponsored Women’s Ischemia Syndrome Evaluation. Journal of the American Heart Association, 8(12), e012406.
https://pubmed.ncbi.nlm.nih.gov/31165670
Masana L, Zamora A, Plana N, et al. Incidence of Cardiovascular Disease in Patients with Familial Hypercholesterolemia Phenotype: Analysis of 5 Years Follow-Up of Real-World Data from More than 1.5 Million Patients. J Clin Med. 2019;8(7):1080. Published 2019 Jul 23. doi:10.3390/jcm8071080
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6678686
Mendieta, Guiomar, Stuart Pocock, Virginia Mass, Andrea Moreno, Ruth Owen, Inés García-Lunar, Beatriz López-Melgar, et al. 2023. “Determinants of Progression and Regression of Subclinical Atherosclerosis Over 6 Years.” Journal of the American College of Cardiology 82 (22): 2069–83.
https://pubmed.ncbi.nlm.nih.gov/37993199
Navar, A. M., Fine, L. J., Ambrosius, W. T., Brown, A., Douglas, P. S., Johnson, K., … & Lewis, C. E. (2022). Earlier treatment in adults with high lifetime risk of cardiovascular diseases: what prevention trials are feasible and could change clinical practice? Report of a National Heart, Lung, and Blood Institute (NHLBI) workshop. American journal of preventive cardiology, 12, 100430.
https://pubmed.ncbi.nlm.nih.gov/36439649
O’Donoghue, M. L., Rosenson, R. S., Gencer, B., López, J. A. G., Lepor, N. E., Baum, S. J., … & Sabatine, M. S. (2022). Small interfering RNA to reduce lipoprotein (a) in cardiovascular disease. New England Journal of Medicine, 387(20), 1855-1864.
https://www.nejm.org/doi/full/10.1056/NEJMoa2211023
Orio Jr, F., Palomba, S., Cascella, T., De Simone, B., Di Biase, S., Russo, T., … & Colao, A. (2004). Early impairment of endothelial structure and function in young normal-weight women with polycystic ovary syndrome. The Journal of Clinical Endocrinology & Metabolism, 89(9), 4588-4593.
https://pubmed.ncbi.nlm.nih.gov/15356067
Osibogun O, Ogunmoroti O, Michos ED. Polycystic ovary syndrome and cardiometabolic risk: Opportunities for cardiovascular disease prevention. Trends Cardiovasc Med. 2020;30(7):399-404. doi:10.1016/j.tcm.2019.08.010
https://www.sciencedirect.com/science/article/pii/S1050173819301288?via%3Dihub
Pletcher MJ, Vittinghoff E, Thanataveerat A, Bibbins-Domingo K, Moran AE. Young Adult Exposure to Cardiovascular Risk Factors and Risk of Events Later in Life: The Framingham Offspring Study. PLoS One. 2016;11(5):e0154288. Published 2016 May 3. doi:10.1371/journal.pone.0154288
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4854462
Powell-Wiley, T. M., Poirier, P., Burke, L. E., Després, J. P., Gordon-Larsen, P., Lavie, C. J., … & American Heart Association Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Epidemiology and Prevention; and Stroke Council. (2021). Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation, 143(21), e984-e1010.
https://pubmed.ncbi.nlm.nih.gov/33882682
Safford, M. M., Gamboa, C. M., Durant, R. W., Brown, T. M., Glasser, S. P., Shikany, J. M., … & Muntner, P. (2015). Race–Sex Differences in the Management of Hyperlipidemia: The REasons for Geographic And Racial Differences in Stroke Study. American journal of preventive medicine, 48(5), 520-527.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4422177
Talbott EO, Zborowski JV, Rager JR, Boudreaux MY, Edmundowicz DA, Guzick DS. Evidence for an association between metabolic cardiovascular syndrome and coronary and aortic calcification among women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2004;89(11):5454-5461. doi:10.1210/jc.2003-032237
https://academic.oup.com/jcem/article/89/11/5454/2844369?login=false
Wilson DP, Jacobson TA, Jones PH, et al. Use of Lipoprotein(a) in clinical practice: A biomarker whose time has come. A scientific statement from the National Lipid Association [published correction appears in J Clin Lipidol. 2022 Sep-Oct;16(5):e77-e95]. J Clin Lipidol. 2019;13(3):374-392. doi:10.1016/j.jacl.2019.04.010
https://www.lipidjournal.com/article/S1933-2874(22)00244-6/fulltext#seccesectitle0006
392 επεισόδια
Manage episode 433043550 series 2585945
Το περιεχόμενο παρέχεται από το CardioNerds. Όλο το περιεχόμενο podcast, συμπεριλαμβανομένων των επεισοδίων, των γραφικών και των περιγραφών podcast, μεταφορτώνεται και παρέχεται απευθείας από τον CardioNerds ή τον συνεργάτη της πλατφόρμας podcast. Εάν πιστεύετε ότι κάποιος χρησιμοποιεί το έργο σας που προστατεύεται από πνευματικά δικαιώματα χωρίς την άδειά σας, μπορείτε να ακολουθήσετε τη διαδικασία που περιγράφεται εδώ https://el.player.fm/legal.
CardioNerds Dan Ambinder and Dr. Devesh Rai join cardiology fellows and National Lipid Association lipid scholars Dr. Oby Ibe from Temple University and Dr. Elizabeth Epstein from Scripps Clinic. They discuss a case involving a patient with elevated Lp(a). Dr. Jessica Pena provides expert commentary. Drs. Oby Ibe and Elizabeth Epstein drafted notes. CardioNerds Intern Christiana Dangas engineered episode audio. This episode is part of a case reports series developed in collaboration with the National Lipid Association and their Lipid Scholarship Program, with mentorship from Dr. Daniel Soffer and Dr. Eugenia Gianos.
An asymptomatic 34-year-old female presented to the cardiology clinic for cardiovascular risk assessment. Her past medical history included polycystic ovarian syndrome (PCOS) and depression. Her labs were notable for total cholesterol 189 mg/dL, LDL of 131 mg/dL, HDL 34 mg/dL, triglycerides 134 mg/dL, and Lp(a) 217 nmol/L. Her 10-year ASCVD risk by the PREVENT calculator was 0.5%, and her 30-year risk was 3.5%. She had no carotid plaque. Because her 30-year risk was significantly increased by her elevated Lp(a), intensive risk factor management was emphasized, and she was started on a low-dose statin with a plan to follow the patient to reassess the need for intensification of lipid-lowering and/or initiation of novel Lp(a)-lowering therapies over time.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
Pearls – Little (a), Big Deal – National Lipid Association
- You are never too young to see a preventive cardiologist! The field of preventive cardiology is shifting focus towards the identification of early upstream risk and intervention before the development of clinical ASCVD (1,5). Patients who have a strong family history of cardiovascular disease, a personal history of CVD at an early age, multiple risk factors, or genetic disorders such as familial hypercholesterolemia especially benefit from early cardiovascular risk assessment and reduction.
- Female-specific risk factors to incorporate into a young woman’s cardiovascular risk assessment include polycystic ovarian syndrome, hormone contraceptive use, early menarche (age <10 years old), primary ovarian insufficiency, fertility therapy, hypertensive disorders of pregnancy (eclampsia, preeclampsia, gestational hypertension, preterm delivery, gestational diabetes, multi-parity >5 pregnancies), early menopause (age <45 years old), & post-menopausal hormone therapy.
- Lp(a) testing for all! The most recent NLA scientific statement on the use of Lp(a) in clinical practice recommends measuring Lp(a) at least once in every adult for risk stratification.
- While Lp(a) has not yet been incorporated into our risk calculators, we do know that elevated Lp(a) increases 10-year risk. The European Atherosclerosis Society published a consensus statement on Lp(a), which includes a handy table to quantify the degree to which a patient’s 10-year risk increases as Lp(a) increases.
- Lifestyle changes are the first line and can reduce the risk of high Lp(a) by 66%. Next, we can consider the risks and benefits of LDL-lowering in a young patient and monitor closely for the development of plaque over time. Lp(a) lowering drugs such as olpasiran are on the horizon, and we can keep this patient in mind as a potential candidate for therapy in the future.
Notes – Little (a), Big Deal – National Lipid Association
When should patients see a preventive cardiologist?
- Strong family history of cardiovascular disease – A positive family history of CVD was defined as a self‐reported diagnosis of CVD in parents, siblings, or children that occurred at 60 years or younger. A positive family history of CVD is an independent predictor of both myocardial infarction and stroke. Among individuals with hypertension, family history of CVD has been shown to be independently associated with mortality by ischemic heart disease and family history of CVD mortality with incidence of overall CVD. Family history of CVD modifies future CVD risk depending on the number and age of affected first-degree relatives. Siblings of patients with CVD have about a 40% risk increase, while offspring of parents with premature CVD have a 60% to 75% risk increase.
- Personal history of early CVD – A personal history of cardiovascular disease at an age younger than 60 years. For young and middle-aged adults, increases in heart disease between 2020 and 2021 explain more than 4% of the most recent shortening in life expectancy. In particular, hypertensive heart disease, heart failure, and endocarditis have increased in young adults, particularly among Black individuals, through 2018. Consequently, young adults make up a growing proportion of cardiovascular disease events, with the proportion of premature myocardial infarction among adults younger than 40 years increasing by 2% every year. The increasing event rates observed among younger adults can be attributed to the increasing prevalence and onset of risk factors such as obesity and hypertension at younger ages, which exacerbate cumulative exposure and cardiovascular disease risk over near- and long-term time horizons.
- Multiple cardiovascular risk factors – Risk factors include hyperlipidemia, high triglycerides, elevated lp(a), diabetes mellitus, obesity, tobacco use, unhealthy diet, and lack of physical activity. Unadjusted event rates were 8-fold to 30-fold higher in persons with adverse levels of risk factor exposure during young adulthood (age 20–39 years) compared with persons with optimal levels of exposure.
- Familial hypercholesterolemia – In primary prevention, patients with FH had incidences of ASCVD and coronary heart disease (CHD) of 14.9/1000 and 5.8/1000 person-years, respectively, compared to 7.1/1000 and 2.1/1000 person-years in the normolipidemic group. FH conferred a hazard ratio (HR) of 7.1 and 16.7 for ASCVD and CHD, respectively, in patients younger than 35 years. In secondary prevention, patients with FH had incidences of ASCVD and CHD of 89.7/1000 and 34.5/1000 person-years, respectively, compared to 90.9/1000 and 28.2/1000 person-years in the normolipidemic group
What are some female-specific risk factors for cardiovascular disease? (7)
- PCOS – Polycystic ovarian syndrome (PCOS) is a disorder characterized by hyperandrogenism and menstrual irregularities. Women affected by PCOS have a heightened risk of developing diabetes due to associated insulin resistance, central obesity, and hypertension. This adverse cardiovascular risk profile in women with PCOS may lead to premature atherosclerosis (8,20). Women with PCOS have been shown to have an increased risk for CVD events (21).
- Depression — Among 593,616 young adults (aged 18–49 years) from 2017 to 2020, depression was independently associated with CHD and suboptimal cardiovascular health (CVH), with a dose‐response relationship (CVH was determined using 7 cardiovascular risk factors: hypertension, hypercholesterolemia, overweight/obesity, current smoking, diabetes, physical inactivity, and inadequate fruit and vegetable intake) (13). Suboptimal CVH was defined as the presence of ≥2 of these 7 cardiovascular risk factors, whereas optimal CVH was 0 or 1 cardiovascular risk factor.
- Early menarche – Results from the Women’s Ischemia Syndrome Evaluation (WISE) study demonstrated that in comparison to women with menarche at age 12 years, there was an approximately 4-fold adjusted increased risk for major adverse cardiac events for menarche ≤ 10 years (15).
- African descent – Safford et al. found that among those at the highest CHD risk, Black women’s hyperlipidemia was the least likely to be treated or controlled. Lp(a) is significantly higher among Blacks versus Whites, and in both, increased Lp(a) correlates positively with LDL-C and negatively with triglycerides. Another study based on the MESA population demonstrated that Black participants showed a significant risk of CHD in those with Lp(a) levels ≥ 75 nmol/L as opposed to White and Hispanic participants who had a greater risk with Lp(a) levels ≥125 nmol/L.
- Elevated BMI – Obesity and higher measures of central adiposity are associated with significantly higher rates of CAD, CVD mortality, sudden cardiac death, heart failure, and arrhythmias (23). High BMI accounted for 4.0 million deaths in 2015, more than two-thirds of which were caused by cardiovascular disease. Marked increases in obesity prevalence among adolescents over the past 35 years ultimately contribute to CVD risk into young adulthood.
Who should be getting an Lp(a) measured?
- Per the most NLA-focused update to the 2019 scientific statement on the use of Lp(a) in clinical practice, we now have sufficient evidence to support measuring Lp(a) at least once in all adults for risk stratification.
What risk calculators would apply to a young adult?
- The American Heart Association recently released the PREVENT calculator (c-statistic 0.72) for 10- and 30-year risk estimation of total CVD (composite of atherosclerotic CVD and heart failure) in primary prevention patients (10). This improves upon the prior pooled cohort equation because it is based on newer data from a larger, more diverse sample (6,612,004 US adults 30 to 79 years of age) than the existing tool. The calculator also takes into account other health conditions, such as cardiovascular-kidney-metabolic risk factors, adjusts for competing risk of non-CVD death, and incorporates an indicator of social determinants of health. Race was not included because it is a social construct, not a biological risk factor, and could, therefore, create bias. Three research teams were awarded $150,000 from AHA to further study how the risk calculator performs among people of various ages, racial and ethnic backgrounds, locations, and socioeconomic levels.
- A universal calculator (c-statistic 0.747 and 0.691 for patients with and without CAD) was also recently published in JACC. This was unique because it can be used in patients both with and without CAD, doing away with the concepts of primary vs secondary prevention and placing everyone on the same spectrum of risk. The calculator incorporates ASCVD vs no ASCVD, age, diabetes, SBP, HTN treatment, TC, smoking history, CRP, NT Pro-BNP, hs Troponin T and provides a 5- and 10-year risk of MACE. The calculator was able to identify patients without CAD who had a higher risk than those with prior CAD. This calculator is not yet available online, but the authors did publish their formulae, which can be plugged into Excel to create a calculator. Unfortunately, this calculator may not apply to our patient because it was validated in a cohort of patients aged 45-64 years.
- QRISK3 (c-statistic 0.75) has been validated in patients aged 25-84 years, so it can be useful in predicting cardiovascular disease in both younger and older patients. It also incorporates a wider variety of risk-enhancing factors than most other calculators, including diagnosis of HIV/AIDS, inflammatory diseases, CKD stage, type 1 and type 2 diabetes, and erectile dysfunction. However, it is important to note that this calculator was validated in a primarily European population, and the risk prediction may not be as accurate in other ethnic groups.
How does elevated Lp(a) influence a patient’s 10-year risk, and can we quantify it?
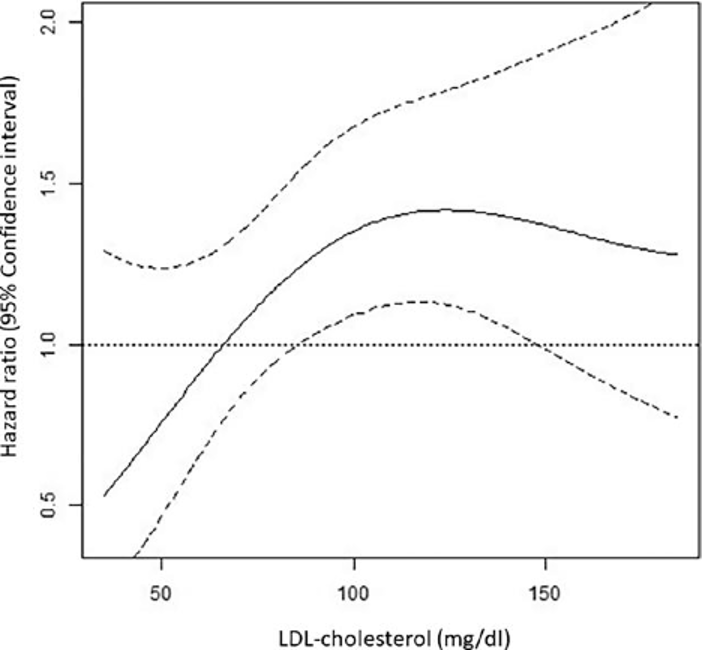
- A recent observational study demonstrated that elevated Lp(a) is associated with long-term MACE in both patients with and without cardiovascular disease. Among patients with ASCVD, individuals in the 71st to 90th percentile group had a 21% increased hazard of MACE (adjusted HR: 1.21; P < 0.001), and among patients without ASCVD, individuals in the 91st to 100th Lp(a) percentile group had the highest relative risk with an adjusted HR of 1.93 (P < 0.001). In patients without ASCVD, there was a linear association between Lp(a) and CV events, whereas in patients with prior ASCVD, the association plateaued between 150-200 nmol/L.
- Similarly, the 2019 consensus statement from HEART UK categorized the impact of CV risk associated with Lp(a) as minor, moderate, high, or very high based on the level of Lp(a). The table from this paper is a clinically useful tool to categorize risk from Lp(a).
- The European Atherosclerosis Society has published a consensus statement on Lp(a) in the European Heart Journal which includes another useful table to adjust a patient’s 10-year risk based on the Lp(a) level(12).
How do we manage a young patient with elevated Lp(a)? Which patients might benefit from treatment with emerging Lp(a)-lowering therapies?
- Given we do not yet have Lp(a) lowering therapies available for clinical use, the mainstay of management for patients with elevated Lp(a) is intensive risk factor management. Beyond the question of LDL lowering, we know that lifestyle change plays a big role in patients with elevated Lp(a) specifically. While it was previously thought that lifestyle has no impact on ASCVD risk associated with elevated Lp(a), in fact, it very much does. It doesn’t lower Lp(a) directly but following the AHA Life’s Simple 8 lowers the risk of Lp(a) by 66%.
- There is some newer data suggesting that in patients with coronary artery disease, aggressive LDL lowering down to 50 can reduce the risk of Lp(a) by up to 50% (6). LDL of 50 mg/dL is a pretty aggressive treatment goal, which makes sense in very high-risk patients with existing CAD. However, we still need more data to guide LDL treatment goals in young patients(18).
- Novel Lp(a)-lowering therapies such as olpasiran are currently in clinical trials (19). We await the data from these trials in order to understand which patients would benefit most from treatment.
References
Allen N, Wilkins JT. The Urgent Need to Refocus Cardiovascular Disease Prevention Efforts on Young Adults. JAMA. 2023;329(11):886-887. doi:10.1001/jama.2023.2308
https://jamanetwork.com/journals/jama/fullarticle/2802264
Baber, Usman, Roxana Mehran, Samantha Sartori, Mikkel Malby Schoos, Henrik Sillesen, Pieter Muntendam, Mario J. Garcia, et al. 2015. “Prevalence, Impact, and Predictive Value of Detecting Subclinical Coronary and Carotid Atherosclerosis in Asymptomatic Adults: The BioImage Study.” Journal of the American College of Cardiology 65 (11): 1065–74.
https://pubmed.ncbi.nlm.nih.gov/25790876
Bhatia, H. S., Trainor, P., Carlisle, S., Tsai, M. Y., Criqui, M. H., DeFilippis, A., & Tsimikas, S. (2024). Aspirin and Cardiovascular Risk in Individuals With Elevated Lipoprotein (a): The Multi‐Ethnic Study of Atherosclerosis. Journal of the American Heart Association, 13(3), e033562.
https://www.ahajournals.org/doi/10.1161/JAHA.123.033562
Coll, B., Betriu, A., Feinstein, S. B., Valdivielso, J. M., Zamorano, J. L., & Fernandez, E. (2013). The role of carotid ultrasound in assessing carotid atherosclerosis in individuals at low-to-intermediate cardiovascular risk. Revista Española de Cardiología (English Edition), 66(12), 929-934.
https://pubmed.ncbi.nlm.nih.gov/24774105
Devesa, A, Ibanez, B, Malick, W. et al. Primary Prevention of Subclinical Atherosclerosis in Young Adults: JACC Review Topic of the Week. J Am Coll Cardiol. 2023 Nov, 82 (22) 2152–2162.
https://www.jacc.org/doi/10.1016/j.jacc.2023.09.817
Dykun, Iryna, Jürgen Kampf, Tienush Rassaf, and Amir A. Mahabadi. 2023. “Interaction between Elevated Lipoprotein(a) and LDL Cholesterol on Mortality Risk in Patients with Coronary Artery Disease.” European Journal of Preventive Cardiology 30 (13): e64–65.
https://academic.oup.com/eurjpc/article-abstract/30/13/e64/7065497?redirectedFrom=PDF
Elder P, Sharma G, Gulati M, Michos ED. Identification of female-specific risk enhancers throughout the lifespan of women to improve cardiovascular disease prevention. Am J Prev Cardiol. 2020;2:100028. Published 2020 Jun 6. doi:10.1016/j.ajpc.2020.100028
https://www.sciencedirect.com/science/article/pii/S2666667720300283
Glintborg D, Rubin KH, Nybo M, Abrahamsen B, Andersen M. Cardiovascular disease in a nationwide population of Danish women with polycystic ovary syndrome. Cardiovasc Diabetol. 2018;17(1):37. Published 2018 Mar 8. doi:10.1186/s12933-018-0680-5
https://pubmed.ncbi.nlm.nih.gov/29519249
Guan, W., Cao, J., Steffen, B. T., Post, W. S., Stein, J. H., Tattersall, M. C., … & Tsai, M. Y. (2015). Race is a key variable in assigning lipoprotein (a) cutoff values for coronary heart disease risk assessment: the Multi-Ethnic Study of Atherosclerosis. Arteriosclerosis, thrombosis, and vascular biology, 35(4), 996-1001.
https://pubmed.ncbi.nlm.nih.gov/25810300
Khan, S. S., Coresh, J., Pencina, M. J., Ndumele, C. E., Rangaswami, J., Chow, S. L., … & American Heart Association. (2023). Novel prediction equations for absolute risk assessment of total cardiovascular disease incorporating cardiovascular-kidney-metabolic health: a scientific statement from the American Heart Association. Circulation, 148(24), 1982-2004.
https://www.ahajournals.org/doi/10.1161/CIR.0000000000001191
Kolber MR, Scrimshaw C. Family history of cardiovascular disease. Can Fam Physician. 2014;60(11):1016.
Kronenberg, Florian, Samia Mora, Erik S. G. Stroes, Brian A. Ference, Benoit J. Arsenault, Lars Berglund, Marc R. Dweck, et al. 2022. “Lipoprotein(a) in Atherosclerotic Cardiovascular Disease and Aortic Stenosis: A European Atherosclerosis Society Consensus Statement.” European Heart Journal 43 (39): 3925–46.
https://pubmed.ncbi.nlm.nih.gov/36036785
Kwapong YA, Boakye E, Khan SS, et al. Association of Depression and Poor Mental Health With Cardiovascular Disease and Suboptimal Cardiovascular Health Among Young Adults in the United States. J Am Heart Assoc. 2023;12(3):e028332. doi:10.1161/JAHA.122.028332
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9973664
Lau, F. D., & Giugliano, R. P. (2022). Lipoprotein (a) and its significance in cardiovascular disease: a review. Jama Cardiology.
https://pubmed.ncbi.nlm.nih.gov/35583875
Lee, J. J., Cook‐Wiens, G., Johnson, B. D., Braunstein, G. D., Berga, S. L., Stanczyk, F. Z., … & Shufelt, C. L. (2019). Age at menarche and risk of cardiovascular disease outcomes: findings from the National Heart Lung and Blood Institute‐sponsored Women’s Ischemia Syndrome Evaluation. Journal of the American Heart Association, 8(12), e012406.
https://pubmed.ncbi.nlm.nih.gov/31165670
Masana L, Zamora A, Plana N, et al. Incidence of Cardiovascular Disease in Patients with Familial Hypercholesterolemia Phenotype: Analysis of 5 Years Follow-Up of Real-World Data from More than 1.5 Million Patients. J Clin Med. 2019;8(7):1080. Published 2019 Jul 23. doi:10.3390/jcm8071080
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6678686
Mendieta, Guiomar, Stuart Pocock, Virginia Mass, Andrea Moreno, Ruth Owen, Inés García-Lunar, Beatriz López-Melgar, et al. 2023. “Determinants of Progression and Regression of Subclinical Atherosclerosis Over 6 Years.” Journal of the American College of Cardiology 82 (22): 2069–83.
https://pubmed.ncbi.nlm.nih.gov/37993199
Navar, A. M., Fine, L. J., Ambrosius, W. T., Brown, A., Douglas, P. S., Johnson, K., … & Lewis, C. E. (2022). Earlier treatment in adults with high lifetime risk of cardiovascular diseases: what prevention trials are feasible and could change clinical practice? Report of a National Heart, Lung, and Blood Institute (NHLBI) workshop. American journal of preventive cardiology, 12, 100430.
https://pubmed.ncbi.nlm.nih.gov/36439649
O’Donoghue, M. L., Rosenson, R. S., Gencer, B., López, J. A. G., Lepor, N. E., Baum, S. J., … & Sabatine, M. S. (2022). Small interfering RNA to reduce lipoprotein (a) in cardiovascular disease. New England Journal of Medicine, 387(20), 1855-1864.
https://www.nejm.org/doi/full/10.1056/NEJMoa2211023
Orio Jr, F., Palomba, S., Cascella, T., De Simone, B., Di Biase, S., Russo, T., … & Colao, A. (2004). Early impairment of endothelial structure and function in young normal-weight women with polycystic ovary syndrome. The Journal of Clinical Endocrinology & Metabolism, 89(9), 4588-4593.
https://pubmed.ncbi.nlm.nih.gov/15356067
Osibogun O, Ogunmoroti O, Michos ED. Polycystic ovary syndrome and cardiometabolic risk: Opportunities for cardiovascular disease prevention. Trends Cardiovasc Med. 2020;30(7):399-404. doi:10.1016/j.tcm.2019.08.010
https://www.sciencedirect.com/science/article/pii/S1050173819301288?via%3Dihub
Pletcher MJ, Vittinghoff E, Thanataveerat A, Bibbins-Domingo K, Moran AE. Young Adult Exposure to Cardiovascular Risk Factors and Risk of Events Later in Life: The Framingham Offspring Study. PLoS One. 2016;11(5):e0154288. Published 2016 May 3. doi:10.1371/journal.pone.0154288
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4854462
Powell-Wiley, T. M., Poirier, P., Burke, L. E., Després, J. P., Gordon-Larsen, P., Lavie, C. J., … & American Heart Association Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Epidemiology and Prevention; and Stroke Council. (2021). Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation, 143(21), e984-e1010.
https://pubmed.ncbi.nlm.nih.gov/33882682
Safford, M. M., Gamboa, C. M., Durant, R. W., Brown, T. M., Glasser, S. P., Shikany, J. M., … & Muntner, P. (2015). Race–Sex Differences in the Management of Hyperlipidemia: The REasons for Geographic And Racial Differences in Stroke Study. American journal of preventive medicine, 48(5), 520-527.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4422177
Talbott EO, Zborowski JV, Rager JR, Boudreaux MY, Edmundowicz DA, Guzick DS. Evidence for an association between metabolic cardiovascular syndrome and coronary and aortic calcification among women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2004;89(11):5454-5461. doi:10.1210/jc.2003-032237
https://academic.oup.com/jcem/article/89/11/5454/2844369?login=false
Wilson DP, Jacobson TA, Jones PH, et al. Use of Lipoprotein(a) in clinical practice: A biomarker whose time has come. A scientific statement from the National Lipid Association [published correction appears in J Clin Lipidol. 2022 Sep-Oct;16(5):e77-e95]. J Clin Lipidol. 2019;13(3):374-392. doi:10.1016/j.jacl.2019.04.010
https://www.lipidjournal.com/article/S1933-2874(22)00244-6/fulltext#seccesectitle0006
392 επεισόδια
Tous les épisodes
×Καλώς ήλθατε στο Player FM!
Το FM Player σαρώνει τον ιστό για podcasts υψηλής ποιότητας για να απολαύσετε αυτή τη στιγμή. Είναι η καλύτερη εφαρμογή podcast και λειτουργεί σε Android, iPhone και στον ιστό. Εγγραφή για συγχρονισμό συνδρομών σε όλες τις συσκευές.
Παρόμοιες με Cardionerds: A Cardiology Podcast
Introducing the BODi® Partner Podcast, the official podcast channel devoted exclusively to BODi Partners. From archives of the BODi Wake-Up Call, I Am BODi stories, and What I Know Now success tips from seasoned Partners, this podcast is your one-stop source for personal development, business training and peer-to-peer inspiration. Ready to explode your business? Tune in regularly to our official podcast and join the ranks of those transforming their lives and the lives of others!
…
continue reading
We are often distracted in life and never really dive deep into the real foundation of self improvement, goal achieving, and wellbeing. - Join our team of experts every week as we discuss the real facets of manhood. Topics like: How to develop more self esteem, self love, deeper relationships. How to improve our wellbeing, mental toughness, resilience, and productivity. How to develop critical skills, become better leaders, expand our careers/business, create financial security and contribut ...
…
continue reading
Although the world is becoming mostly sedentary, our bodies still require a wide variety of daily movements in order to work well. Many of us struggle to get regular exercise, but even that can fall short of nourishing the body from head to toe. How can we move more—a lot more—when we have sore, stiff parts and overly busy lifestyles? Join Katy Bowman M.S., biomechanist, author, and movement educator as she combines big-picture lessons on biomechanics, kinesiology, physiology, and natural hu ...
…
continue reading
For the complete newbie or the experienced hypnotist, Brain Software with Mike Mandel is the world's most interesting, educational and fun podcast discussing hypnosis, NLP and strategies for peak performance and self improvement. Mike Mandel is a 6-time award winning hypnotist, immensely popular keynote speaker, stage performer, psychotherapist and NLP trainer. He has been doing hypnosis since he was 12 years old. Mike has an amazing ability to demystify hypnosis, teach core concepts, and te ...
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
Practical herbalism from practicing herbalists. Conversations, botanical deep-dives, Q&A with clinical herbalists Katja Swift & Ryn Midura of CommonWealth Holistic Herbalism.
…
continue reading
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Welcome to Almost 30 - a supportive space to fuel your conscious evolution. Join us, LA-based best friends Krista Williams and Lindsey Simcik, for heart-centered, hilarious conversations and real, raw, impactful interviews with brilliant guests. We dive deep into topics like modern spirituality to health and wellness, aliens to entrepreneurship, social justice, and self development. With every episode, our mission is to empower you, expand what you think is possible and, make you laugh - a l ...
…
continue reading
Short guided meditations to calm your anxiety, overcome negative thinking, increase your confidence, and more. Don’t think you have the time, or mental focus, to meditate? Most of these mind-shifting meditations are 10 minutes or less. Soothe your stress away and feel better fast with this award winning guided meditation podcast by Hypnotherapist Chel Hamilton today. For more information visit: https://meditationminis.com (https://meditationminis.com/) Please Note: The meditations presented ...
…
continue reading
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
Player FM - Εφαρμογή podcast
Πηγαίνετε εκτός σύνδεσης με την εφαρμογή Player FM !
Πηγαίνετε εκτός σύνδεσης με την εφαρμογή Player FM !



